

If you’ve ever gotten a blood test back, you’re familiar with the routine. You scan the list, see your numbers fall within or near the "standard range," and your doctor gives you a thumbs-up and says you are “normal” before sending you on your way.
But for those of us serious about optimizing our health or achieving peak performance a critical question arises: Is "normal" good enough?
In reality, the "normal" range on your lab report is typically just a statistical average of the population, however, the average health status of people across the globe is in rapid decline as seen by rises in diseases like: diabetes, heart disease, cancer, and neurodegenerative disease.
| Disease Category | Key Trend Statistic | Timeframe | Primary Source Cited |
|---|---|---|---|
| Diabetes | Prevalence increased from 7% to 14% of adults | 1990–2022 | World Health Organization (WHO) |
| Heart Disease | Prevalence of Ischemic Heart Disease increased by 226.7% | 1990–2021 | Global Burden of Disease (GBD) 2021 |
| Cancer | Annual new cases projected to increase by 77% | 2022–2050 | IARC (GLOBOCAN 2022) |
| Neurodegenerative | Prevalence of Alzheimer's & Dementias increased by 160.84% | 1990–2019 | Global Burden of Disease (GBD) 2019 |
This is where proactive health monitoring becomes essential. While our system is often reactive, the data to be proactive is readily available.
If you are looking to start collecting your own data I personally use and highly recommend GoodLabs. They have best prices I have found and also allow people to donate blood while getting free blood test results which is awesome for everyone.
The good news is we do have data and studies that show what "optimal" ranges are for many biomarkers. We can dive into more detail here in the future but for now the optimal ranges shared below are associated with longer life spans as well as a reduction in chronic diseases.
Let’s dive into the most critical blood tests for optimal health, what the ideal ranges are, and why they matter.
1. ApoB (Apolipoprotein B): The True Driver of Heart Disease
What it is: Forget the old standard LDL cholesterol for understanding cardiovascular disease risk. Apolipoprotein B (ApoB) is a direct measure of the number of all atherogenic (plaque-causing) lipoprotein particles in your bloodstream, making it the most accurate predictor of cardiovascular disease risk. Think of it as a traffic count for your arteries—while LDL-C measures the cargo in the cars, ApoB counts the total number of cars. The more cars on the road, the higher the chance of a "traffic jam" that leads to plaque buildup.
- Standard "Normal" Range: < 130 mg/dL
- Longevity Optimal: < 60 mg/dL
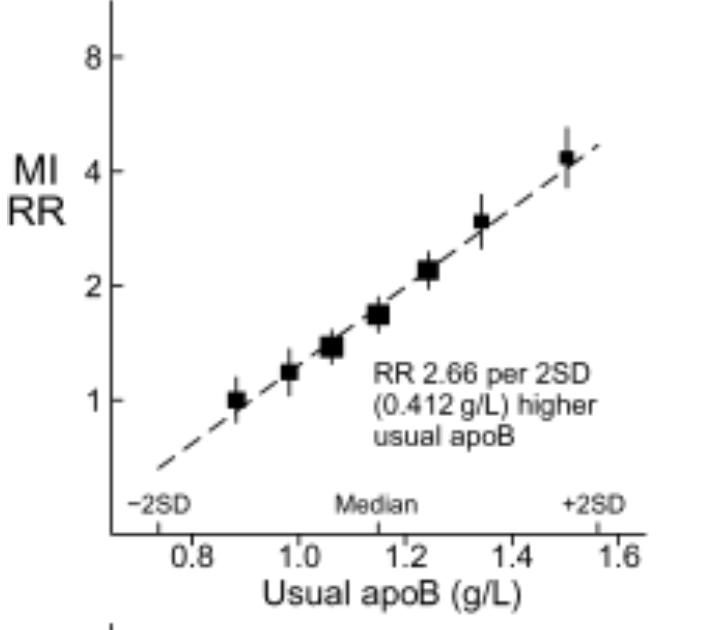
The Science: The evidence linking ApoB to atherosclerotic cardiovascular disease (ASCVD) is overwhelming. A massive 2020 consensus statement from the European Atherosclerosis Society concluded that ApoB-containing lipoproteins are causally linked to ASCVD. The data is so strong that for every 38.7 mg/dL (1 mmol/L) reduction in ApoB, there is a corresponding ~20-25% reduction in the risk of major vascular events. Experts in the longevity space, like Dr. Tom Dayspring, often advocate for getting this number as low as possible to reduce or potentially eliminate ASCVD risk. As studies like INTERHEART show, there is a direct and powerful correlation between a higher ApoB count and the risk of a heart attack, solidifying its status as the most important metric for cardiovascular risk.
2. hs-CRP (High-Sensitivity C-Reactive Protein): The Silent Fire
What it is: High-sensitivity C-reactive protein (hs-CRP) is a key blood marker that measures chronic, low-grade inflammation throughout your body. This measurement is critical because persistent inflammation is recognized as a major underlying driver of many age-related diseases, including cardiovascular and neurodegenerative conditions.
- Standard "Normal": < 3.0 mg/L
- Longevity Optimal: < 1.0 mg/L (ideally < 0.5 mg/L)
The Science: The link between hs-CRP and cardiovascular risk is well-established. A landmark study published in the New England Journal of Medicine demonstrated that individuals with the highest levels of hs-CRP had a significantly greater risk of heart attack and stroke, independent of other traditional risk factors. For longevity and optimal health, the goal is to maintain the lowest possible level of inflammation. An hs-CRP level below 1.0 mg/L signifies a low inflammatory state, and studies have shown that levels below 0.5 mg/L are associated with the lowest cardiovascular risk.
3. Homocysteine: The Unsung Risk Factor
What it is: Homocysteine is an amino acid that, when elevated, acts as an irritant to the delicate inner lining of your arteries (the endothelium). This damage can increase your risk for blood clots, cardiovascular events, and has also been linked to cognitive decline. Managing homocysteine is a critical, yet often overlooked, component of maintaining long-term vascular and brain health.
- Standard "Normal": < 15 µmol/L
- Longevity Optimal: < 9 µmol/L
The Science: While often overlooked, a landmark meta-analysis published in JAMA established a strong, graded relationship between homocysteine levels and the risk of ischemic heart disease and stroke. The data demonstrates that higher homocysteine is directly associated with a significantly increased risk of cardiovascular events. The good news is that this marker is often highly responsive to increased intake of key B vitamins, particularly folate (B9), B12, and B6.
4. Metabolic Health: Fasting Insulin & Glucose
What they are: These two markers provide a snapshot of your metabolic health. While fasting glucose shows the amount of sugar in your blood at one moment, fasting insulin reveals how hard your body's pancreas is working to keep that glucose level stable. Chronically high insulin is often the earliest warning sign of metabolic dysfunction, long before blood sugar levels rise.
- Standard "Normal": Glucose < 100 mg/dL; Insulin < 25 µIU/mL
- Longevity Optimal: Glucose 75-90 mg/dL; Insulin < 10 µIU/mL (ideally < 5)
The Science: Chronically elevated fasting insulin, a condition known as hyperinsulinemia, often precedes the development of prediabetes and type 2 diabetes by years or even decades. Research has clearly shown that high fasting insulin is an independent risk factor for cardiovascular disease, various cancers, and all-cause mortality, even in individuals with normal blood glucose. For longevity, the goal is not just to have normal glucose, but to achieve it with the lowest possible insulin level, indicating excellent insulin sensitivity.
Alternatives: One can also look at HbA1c as an alternative, though it can be influenced by factors affecting red blood cell lifespan (like anemia) and is best used for tracking your average blood sugar trends over two to three months. One should aim for an HbA1c <5.1% for an optimal longevity target.
5. Vitamin D: The Sunshine Hormone
What it is: More than just a vitamin, Vitamin D functions as a potent pro-hormone that influences thousands of bodily processes. While it's most famous for promoting bone density, it is also a critical regulator of immune function, inflammation, and cellular growth.
- Standard "Normal": > 30 ng/mL
- Longevity Optimal: 40 - 60 ng/mL (I like to target 50 ng/mL)
The Science: The standard "normal" range for Vitamin D is often based on the minimum level needed to prevent overt bone diseases like rickets. However, research focused on optimal health suggests a higher target is better for longevity. A large-scale meta-analysis published in the BMJ established a clear inverse relationship between Vitamin D levels and all-cause mortality, finding that the lowest risk of death from any cause was seen in individuals with levels between 30-60 ng/mL (75-150 nmol/L).
6. Triglyceride / HDL Ratio: The Simple Litmus Test
What it is: This is a simple yet powerful ratio calculated from your standard lipid panel (Total Triglycerides ÷ HDL). It serves as a surprisingly accurate proxy for insulin resistance and gives crucial insight into the size and density of your LDL particles, a key factor in heart disease risk.
- Standard "Normal": < 4.0
- Longevity Optimal: < 1.5 (ideally < 1.0)
The Science: A high Triglyceride/HDL ratio is a major red flag for metabolic syndrome and is considered a strong, independent predictor of cardiovascular events. A low ratio (ideally approaching 1.0) is a hallmark of excellent metabolic health, suggesting you are highly insulin-sensitive and that your LDL particles are likely the large, "fluffy" (less atherogenic) type. Research published in journals like Circulation has repeatedly validated this ratio as a critical, yet simple, risk marker.
7. Omega-3 Index: Your Cellular Health Scorecard
What it is: This test directly measures the percentage of the key omega-3 fatty acids, EPA and DHA, within your red blood cell membranes. Because it provides a stable, long-term picture of your omega-3 status, it's a powerful indicator of your risk for cardiovascular events and a marker for long-term brain health.
- Standard "Normal": > 4%
- Longevity Optimal: > 8%
The Science: A higher Omega-3 Index is strongly associated with better health outcomes. A landmark prospective study found that individuals with an index of 8% or higher had a significantly lower risk of death from all causes compared to those with an index below 4%. A high index is specifically linked to a dramatically reduced risk of sudden cardiac death and is also associated with better cognitive function and a lower risk of dementia later in life.
Putting It All Together
I know this is a lot to track. After spending hundreds of hours poring over this research for myself, I began helping friends and family make sense of their own lab results. I quickly realized that everyone needed the same thing: a way to translate confusing numbers into a simple, actionable health blueprint.
That’s why I built The Kestrel Report.
It’s a system designed to do all the heavy lifting for you, transforming your standard lab results into a clear guide showing exactly where you can optimize your health for longevity and performance.
It's called the Kestrel Report.
This project is new, and I personally create each report and ensure one walks away with new health insights. To thank the readers who are supporting this work from the beginning, I want to offer you my direct expertise for those not wanting to spend all their evenings combing through NIH papers.
If you're serious about your healthspan, let me do the heavy lifting for you. I guarantee you’ll walk away with newfound clarity and a plan to improve.
Learn more and become an early adopter at KestrelReport.com
Sources
- World Health Organization (WHO) - Referenced in the introduction table for Diabetes statistics.
- Global Burden of Disease (GBD) 2021 Study - Referenced in the introduction table for Heart Disease statistics.
- International Agency for Research on Cancer (IARC) GLOBOCAN 2022 - Referenced in the introduction table for Cancer statistics.
- Global Burden of Disease (GBD) 2019 Study - Referenced in the introduction table for Neurodegenerative Disease statistics.
- ApoB (Causal Link): Ference, B. A., et al. (2020). Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel. European Heart Journal, 41(24), 2459–2472. Link
- ApoB (Risk Reduction): Cholesterol Treatment Trialists’ (CTT) Collaboration. (2010). Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. The Lancet, 376(9753), 1670-1681. Link
- ApoB (INTERHEART Study): Yusuf, S., Hawken, S., Ôunpuu, S., et al. (2004). Lipids, Lipoproteins, and Apolipoproteins as Risk Markers of Myocardial Infarction in 52 Countries (the INTERHEART study): a case-control study. The Lancet, 364(9438), 937-952. Link
- hs-CRP: Ridker, P. M., Hennekens, C. H., Buring, J. E., & Rifai, N. (2000). C-Reactive Protein and Other Markers of Inflammation in the Prediction of Cardiovascular Disease in Women. New England Journal of Medicine, 342(12), 836–843. Link
- Homocysteine: The Homocysteine Studies Collaboration. (2002). Homocysteine and Risk of Ischemic Heart Disease and Stroke: A Meta-analysis. JAMA, 288(16), 2015–2022. Link
- Fasting Insulin & Glucose: Després, J. P., Lamarche, B., Mauriège, P., et al. (1996). Hyperinsulinemia as an Independent Risk Factor for Ischemic Heart Disease. New England Journal of Medicine, 334(15), 952–957. Link
- Vitamin D: Chowdhury, R., Kunutsor, S., Vitezova, A., et al. (2014). Vitamin D and all-cause mortality: a systematic review and meta-analysis of observational studies. BMJ, 348, g1903. Link
- Triglyceride / HDL Ratio: Gaziano, J. M., Hennekens, C. H., O'Donnell, C. J., et al. (1997). Fasting triglycerides, high-density lipoprotein, and risk of myocardial infarction. Circulation, 96(8), 2520–2525. Link
- Omega-3 Index: Harris, W. S., Tintle, N. L., Etherton, M. R., & Vasan, R. S. (2018). Erythrocyte long-chain omega-3 fatty acid levels are inversely associated with all-cause mortality. Journal of Clinical Lipidology, 12(3), 748–757.e2. Link